Occupational therapy helps people of all ages do the daily activities that matter to them. It supports those who face physical, mental, or cognitive challenges. This guide covers what OT is, who it helps, and how it fits into UK health and social care.
Occupational therapy (OT) helps people do the everyday things that matter to them. Getting dressed. Cooking. Going to work. Seeing friends. When illness, injury, disability, or ageing gets in the way, an occupational therapist helps that person find a way forward.
OT carries another name: ergotherapy. That word comes from the Greek ergon, meaning to act and to work. The Health and Care Professions Council (HCPC) regulates all practising occupational therapists in the UK. The Royal College of Occupational Therapists (RCOT) acts as the professional body.
What Does ‘Occupation’ Actually Mean in OT?
In everyday life, occupation means a job. In occupational therapy, it means much more.
An occupation is any activity you want to do, need to do, or are expected to do. The World Federation of Occupational Therapists (WFOT) defines OT as a client-centred health profession that promotes health and wellbeing through occupation. The goal is to help people take part in the activities of everyday life.
One simple idea drives OT: humans are occupational beings. Our activities shape who we are. Occupational science, the academic study of this idea, was founded in 1989 by Elizabeth Yerxa at the University of Southern California.
Occupations fall into three areas:
Self-care: washing, dressing, eating, sleeping, and managing your health.
Productivity: working, studying, volunteering, caring for others, and running a household.
Leisure: socialising, sport, hobbies, and creative activities.
Occupations also cover activities of daily living (ADLs) like bathing and eating. They include instrumental activities of daily living (IADLs) like shopping, managing money, and using transport.
Everyone holds a different set of occupations. These shift across a lifetime. When illness or disability cuts a person off from their usual activities, their sense of identity can crack. OT steps in right there.
OT has deep roots. Around 100 BCE, Greek physician Asclepiades treated mental illness with therapeutic baths, massage, exercise, and music.
The modern profession grew from the moral treatment movement in late 18th-century Europe. Physicians Philippe Pinel and Johann Christian Reil reformed the mental asylum system. They replaced harsh conditions with structured work, leisure, and meaningful activity.
The Arts and Crafts movement between 1860 and 1910 shaped OT further. Crafts gave hospital patients purpose and structure during long recoveries.
In the early twentieth century, American social worker Eleanor Clarke Slagle built the habit training model. She earned the title ‘mother of occupational therapy.’ Her model holds that meaningful routines create balance and wellbeing across work, rest, and leisure.
In March 1917, the National Society for the Promotion of Occupational Therapy (NSPOT) held its first meeting in New York. Founders included William Rush Dunton, Eleanor Clarke Slagle, and Thomas B. Kidner. During World War I, the society trained over 1,200 reconstruction aides to rehabilitate injured soldiers. NSPOT adopted the name occupational therapy in 1921. William Rush Dunton argued that occupation is a basic human need and that occupation is therapeutic.
Occupational Therapy in the United Kingdom
In the UK, the profession took its own path. In 1925, Margaret Barr Fulton became the first US-qualified OT to work here. She took a post at the Aberdeen Royal Hospital. In 1930, Dr Elizabeth Casson opened the first UK school of occupational therapy at Dorset House in Bristol. She built it to support women with mental health conditions.
The Scottish Association of Occupational Therapists formed in 1932. The Association of Occupational Therapists covered the rest of the UK from 1936. Both bodies merged in 1974 to form the Royal College of Occupational Therapists (RCOT).
Occupational science grew as an academic discipline in the 1980s. Elizabeth Yerxa formally founded it in 1989.
What Does an Occupational Therapist Do?
An occupational therapist looks at the gap between what a person can do now and what they want or need to do. The process starts with assessment.
The therapist builds an occupational profile. This captures the person’s history, interests, values, daily routines, and the activities that matter most. It builds a full picture of the person, not just their condition.
All OT practice frameworks, including the Occupational Therapy Practice Framework (OTPF) and the Canadian Practice Process Framework (CPPF), follow three steps: evaluation, intervention, and outcomes.
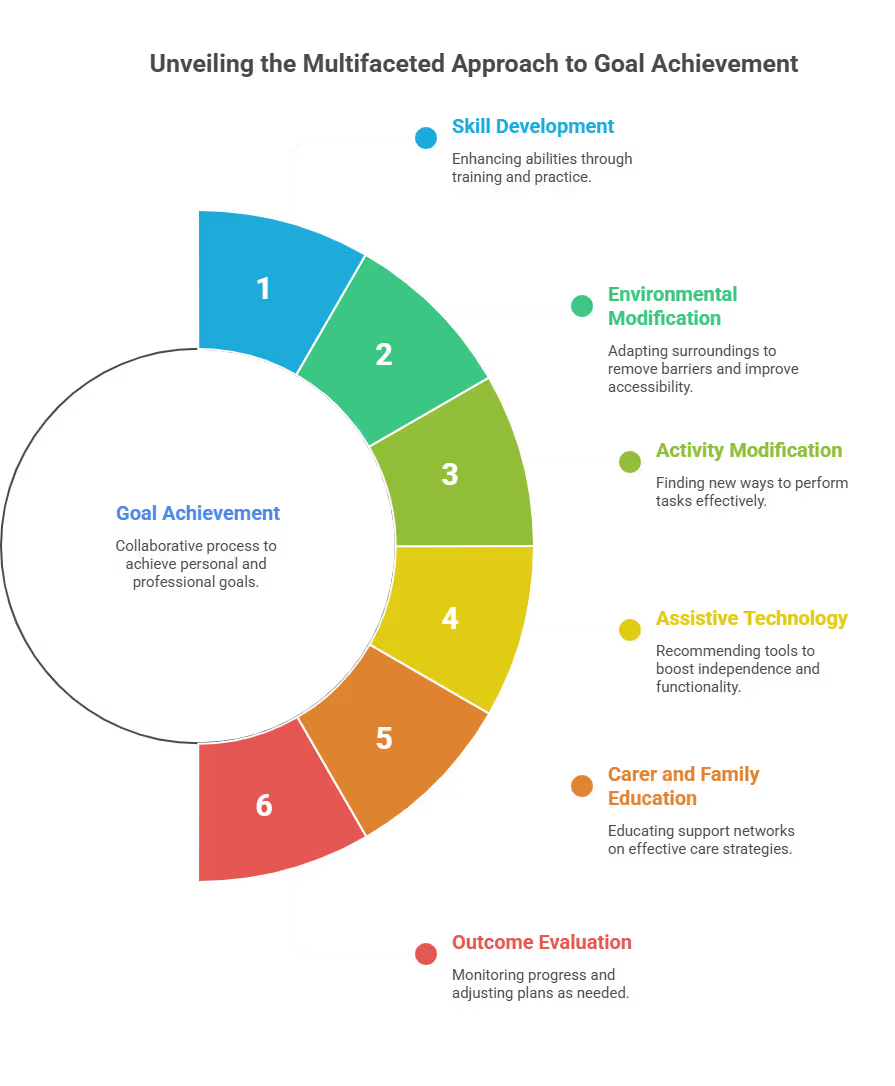
The therapist and the person agree on goals together. A plan is built around those goals. It can include:
Every OT plan follows a client-centred approach. The therapist focuses on the person’s strengths and goals, not their diagnosis. The plan is personal, practical, and built around what the person wants to achieve.
Who Does Occupational Therapy Help?
OT helps people of all ages across a wide range of conditions.
Children and young people: OTs work with children with developmental delays, autism spectrum disorder (ASD), sensory processing disorder, dyspraxia, cerebral palsy, learning disabilities, and other physical or cognitive difficulties. In schools, OTs help children build handwriting skills, manage sensory challenges, and access the curriculum. In early intervention, they work with children under three to support families and promote functional development. Many children receive OT as part of an Education, Health and Care Plan (EHCP) in England.
Working-age adults: OTs support adults who recover from surgery and manage long-term conditions like multiple sclerosis, rheumatoid arthritis, Parkinson’s disease, and cancer. They also help people after stroke, acquired brain injury, or spinal cord injury return to work or education.
Older adults: OTs support older people to stay at home. Key areas include falls prevention, home safety assessments, dementia and Alzheimer’s disease support, aging in place, energy conservation, and driver evaluation.
People with mental health conditions: OTs help people build daily routines, develop coping strategies, and re-engage with meaningful activities as part of a recovery-led approach.
People with physical disabilities: OTs assess functional ability, recommend adaptive equipment and home adaptations, and support people to engage in work, education, and community life.
Marginalised groups: OT reaches refugees, people experiencing homelessness, LGBTQI+ individuals, and those in the justice system. These groups face what OT calls occupational injustice, covered in a dedicated section below.
Key Areas of Occupational Therapy Practice
OT covers many specialist areas. Here are the main ones in the UK.
Paediatric Occupational Therapy
Paediatric OTs work with children in homes, schools, clinics, and hospitals. A core area is sensory integration, a framework A. Jean Ayres developed in the 1960s and 1970s. Sensory integration therapy helps children process sensory input from their body and environment. It builds emotional regulation, motor planning, and participation in school and daily life.
Paediatric OTs also work with neurodivergent children, including those with ASD, ADHD, sensory processing disorder, and dyspraxia. They build fine motor skills, gross motor skills, handwriting, executive function, and social participation.
Mental Health Occupational Therapy
OTs in mental health apply a three-tier public health model. Universal services (Tier 1) promote wellbeing for all. Targeted services (Tier 2) support people at risk. Intensive interventions (Tier 3) support people with identified mental, emotional, or behavioural disorders. Across all tiers, meaningful occupation drives recovery and routine.
This approach aligns with the recovery model. That model helps people with mental health challenges live full, community-based lives and reach their potential. OTs work in inpatient units, community mental health teams, day services, and residential settings.
Adult Rehabilitation
OTs support adults recovering from stroke, acquired brain injury, spinal cord injury, and cancer. Interventions cover cognitive rehabilitation, physical rehabilitation, fatigue management, pressure sore prevention, and training in myoelectric prosthetic limb use. Telehealth also extends OT services to people in rural areas.
Productive Aging and Geriatrics
OTs work with older adults in hospitals, care homes, community settings, and the person’s own home. Key interventions include falls prevention, home modification, dementia support, ADL and IADL retraining, caregiver education, and driver evaluation. The goal is to keep older adults as independent as possible for as long as they choose.
Visual Impairment
OTs support people with low vision and neurological visual impairments like cortical visual impairment (CVI). They modify tasks and environments. They work alongside optometrists and ophthalmologists, especially for people with traumatic brain injury or those aiming to return to driving.
Community-Based Practice
Community OT is now a core part of the profession. OTs work within communities to see the real barriers clients face in their daily environment. They design interventions that fit the person’s actual life, working with families, employers, schools, housing providers, and voluntary organisations.
Nature-Based Therapy
Nature-based interventions form a growing part of OT practice. They include therapeutic gardening, horticultural therapy, and animal-assisted therapy (AAT) with trained dogs, horses, and llamas. Adventure therapy is also used. Evidence shows these approaches build motor skills, cognitive function, emotional regulation, and social engagement, especially for people with ASD and acquired brain injury.
Acute Care
In hospitals, OTs assess whether patients can live independently after discharge. They carry out ADL assessments, recommend adaptive equipment like shower chairs and dressing aids, complete pre-discharge home visits, train carers, and co-ordinate discharge planning as part of a multidisciplinary team (MDT).
Theoretical Frameworks and Practice Models
OT draws on a range of theoretical models. These guide how therapists assess, plan, and deliver care.
Model of Human Occupation (MOHO): Gary Kielhofner first published MOHO in 1980. It explains how people choose, organise, and carry out occupations within their environment. It looks at motivation, habits, roles, and performance capacity. MOHO is one of the most evidenced models in the world.
Person Environment Occupation Performance model (PEOP): Charles Christiansen and M. Carolyn Baum published this in 1991. It looks at how person, environment, occupation, and performance interact. It takes a strengths-based, client-centred approach.
Canadian Model of Occupational Performance and Engagement (CMOP-E): The Canadian Association of Occupational Therapists developed this in 1997. It places the person at the centre with cognitive, affective, and physical components around a spiritual core. The Canadian Practice Process Framework (CPPF) and Canadian Model of Client Centred Enablement (CMCE) sit within this tradition.
Kawa (River) Model: Michael Iwama developed this model. It uses the image of a river to represent a person’s life journey. It applies well across cultures.
Occupational Therapy Practice Framework (OTPF): The OTPF splits OT into domain and process. The domain covers client factors like motivation, health status, and occupational performance. The process covers evaluation, intervention, and outcomes.
International Classification of Functioning, Disability and Health (ICF): The World Health Organisation’s ICF maps health and ability across body function, activity, and participation. OTs use it alongside OT-specific language to describe client needs and progress.
Biopsychosocial model: This model looks at how biological, psychological, and social factors shape a person’s health and occupational performance. It takes a whole-person view.
Sensory integration framework: A. Jean Ayres developed this evidence-based approach. It helps people process sensory input more effectively. Paediatric OTs use it most, especially with children with ASD, sensory processing disorder, and dyspraxia.
Biomechanical frame of reference: This frame focuses on physical motion during occupation. OTs use it with people who face movement, strength, or endurance challenges.
Client-centred frame of reference: Carl Rogers inspired this frame. It puts the client’s goals and values at the heart of all therapy.
Recovery model: This model helps people with mental health challenges live meaningful, community-based lives. OTs use occupation as a route to recovery.
Cognitive-behavioural frame and dynamic systems theory: These frameworks help OTs reason about how thoughts, beliefs, and movement systems shape occupational performance.
The Philosophy Behind Occupational Therapy
OT rests on a distinctive philosophy. The founders drew from romanticism, pragmatism, and humanism. These traditions all value human agency, meaningful activity, and whole-person wellbeing.
Psychiatrist Adolf Meyer shaped the profession early. In 1922, he put forward a holistic view of health that linked daily activity, rhythm, and mental wellbeing. He argued that a balanced mix of work, rest, play, and sleep builds good health.
William Rush Dunton, one of NSPOT’s founders, set out four principles that still drive the profession today:
Occupation builds health and wellbeing.
Occupation creates structure and organises time.
Occupation brings meaning to life, personally and culturally.
Occupations are personal: each person values different activities.
These principles established the core belief that occupation is a basic human need and a therapeutic tool. Holism sits at the heart of the profession. OT looks at the whole person: their environment, relationships, and what they find meaningful, not just their condition.
Over the twentieth century, the profession moved between a clinical, reductionist period and a return to its person-centred roots. Today, client-centredness and the centrality of occupation remain the dominant themes.
What Is Occupational Justice?
Occupational justice is a concept that grew from OT and occupational science. It holds that all people have the right to take part in meaningful occupations. Society carries the duty to remove the barriers that block this.
Occupational injustice happens when people are excluded or deprived of meaningful activities. The WFOT issues position statements on OT’s role in human rights and occupational justice worldwide. Social determinants of health, such as poverty, housing, and discrimination, sit at the centre of how OTs understand this issue.
OT recognises five types of occupational injustice:
Occupational deprivation: External factors block a person from meaningful occupations. A person with mobility difficulties may struggle to access community activities because of poor transport. OTs help by removing environmental barriers and building inclusive programmes.
Occupational apartheid: A person is barred from chosen occupations because of personal characteristics like age, gender, race, or socioeconomic status. OTs address this through environmental modification and occupational exploration.
Occupational marginalisation: Social norms block a person from a chosen occupation. A child with physical impairments may receive only seated activities instead of sport. OTs design inclusive programmes to tackle this.
Occupational imbalance: One occupation blocks participation in others. A family carer may lose access to leisure, employment, or social life. OTs advocate for policies and environments that support balance.
Occupational alienation: Activities are imposed on a person that hold no meaning for them. OTs build personalised, interest-led activities to restore motivation.
OTs also act as advocates. They work with communities, organisations, policymakers, and the World Health Organisation to promote occupational engagement for all, including refugees, people experiencing poverty, individuals with disabilities, and those in the justice system.
How Is Occupational Therapy Regulated in the UK?
The HCPC regulates OT in the UK as one of 15 allied health professions. Across all regulated professions, the HCPC holds 352,593 registrants. In England, allied health professions (AHPs) form the third-largest clinical workforce in health and care.
To use the protected title ‘occupational therapist,’ a person must hold an HCPC-approved qualification and stay registered. Practising without registration is unlawful.
To qualify, a person completes a degree in occupational therapy. This is usually a three-year BSc (Hons) or a two-year postgraduate MSc for those with a relevant first degree. Degree apprenticeships also exist, so people can earn while they train.
Both routes include supervised practice placements, known as fieldwork in global OT education. These give students direct clinical and community experience before they qualify. The World Federation of Occupational Therapists (WFOT) sets minimum education standards worldwide. UK programmes meet HCPC and RCOT accreditation requirements.
After qualifying, NHS occupational therapists join the Agenda for Change (AFC) pay scale, usually starting at Band 5. With experience and further specialist training, OTs move into senior and specialist posts.
The RCOT acts as the professional membership body. It provides guidance, indemnity coverage, and a trade union function. Most practising OTs join.
Registered OTs maintain Continuing Professional Development (CPD) throughout their career. CPD keeps practice current with new evidence, policy, and technology. It includes short courses, peer supervision, conferences, and reflective practice.
Key distinction: a degree and HCPC registration are required to use the title occupational therapist and to practise independently. CPD learning supports professional development but does not grant HCPC registration or the right to practise.
How Is Occupational Therapy Different from Physiotherapy?
People often mix up OT and physiotherapy. Both are regulated allied health professions. Both work together in multidisciplinary teams (MDTs). They are different professions with different focuses.
Physiotherapy targets physical movement, mobility, muscle strength, and cardiorespiratory function. Physiotherapists treat the body’s physical systems.
OT takes a broader view. It looks at how physical, cognitive, emotional, sensory, and environmental factors affect a person’s ability to do the things that matter to them. The focus is on occupational performance and daily life, not physical function alone.
In practice, the two professions work together often. A person recovering from a stroke may work with a physiotherapist to rebuild movement and with an OT to relearn tasks like washing, dressing, and cooking.
Both require a degree and HCPC registration to practise.
Common Misunderstandings About Occupational Therapy
‘OT is only about going back to work.’ Occupation covers all purposeful activity: self-care, leisure, social connection, and productivity. Employment is one occupation among many.
‘OT and physiotherapy are the same.’ They are distinct professions. OT focuses on meaningful daily activity across all areas of life. Physiotherapy focuses on physical function and movement.
‘OT is only for people with physical disabilities.’ OT supports people with mental health conditions, learning disabilities, cognitive difficulties, neurodevelopmental conditions, and age-related challenges too.
‘A CPD course makes you an occupational therapist.’ Practising as an OT requires a degree accredited by the RCOT and HCPC registration. CPD supports professional development. It does not grant registration or the right to practise independently.
‘OT is only available through the NHS.’ OT runs through the NHS, local authority social services, independent practice, voluntary organisations, housing authorities, schools, and the justice system. Access depends on need and circumstances.
‘OT focuses only on the individual.’ OT also works at community and population level. OTs advocate for systemic change, challenge occupational injustice, and shape public health policy.
Quick Recap
OT helps people of all ages do the everyday activities that matter: self-care, work, leisure, and social life. It steps in when illness, injury, disability, or ageing gets in the way.
Occupational therapists must hold a recognised degree and HCPC registration before they can practise. CPD supports professional development but does not replace the initial qualification.
OT rests on holism, client-centredness, and occupational justice, with over a century of theory, occupational science, and evidence behind it.
Studying Through Royal Open College (CPD Learning)
If you work in health or social care, understanding occupational therapy helps you support the people you work with. It also helps you work alongside OT professionals with confidence.
Royal Open College offers CPD learning that covers occupational therapy principles in health and social care settings. The courses cover person-centred care, daily living support, and the OT approach to independence and wellbeing.
These are CPD programmes. They support your learning and professional development. They are not qualifications. They do not lead to HCPC registration or the right to practise as a registered occupational therapist.
For support workers, care assistants, senior carers, and team managers who work alongside OT professionals or support people with daily living needs, this CPD learning builds confidence and a deeper understanding of the people you support.
Heat exhaustion is the body’s warning sign that it is overheating. Heatstroke is a medical emergency. Learn the key differences, early symptoms, first steps, and what UK workplaces and care settings should know during hot weather.
Healthcare assistants and nursing assistants can help keep people safe during a heatwave by supporting hydration, keeping care areas cooler, spotting warning signs early, and reporting concerns quickly. Staff should also protect their own health during hot shifts.
If someone becomes unwell in a heatwave, move them somewhere cool, remove unnecessary clothing, give fluids if safe, cool their skin, and watch closely. Call 999 if you suspect heatstroke or they do not improve after cooling.